
Vaccines by Q3 2026. Oncology by Q4 2026. Mandatory for all new medicines after that. Here is exactly what EMA’s ePI roadmap requires – and the steps to get your organization compliant before deadlines force costly decisions.
In March 2026, the EMA Management Board confirmed: ePI will become mandatory for all newly authorized medicines once the new EU pharmaceutical legislation takes effect. The voluntary phase was a runway – not a permanent option. With the EU Pharmaceutical Package politically agreed in December 2025, that runway is now very short
This article is written for regulatory affairs leads, VP-level compliance owners, and CMC directors at pharma manufacturers holding or pursuing centrally authorized products in the EU – particularly those with vaccine or oncology portfolios
What EMA’s ePI Mandate Actually Requires
The EU ePI Common Standard is built on HL7 FHIR. The SmPC, Package Leaflet, and labelling are structured as machine-readable FHIR resources – not documents – submitted through the EU medicines regulatory network.
The March 2026 EMA ePI implementation roadmap set the following implementation sequence:
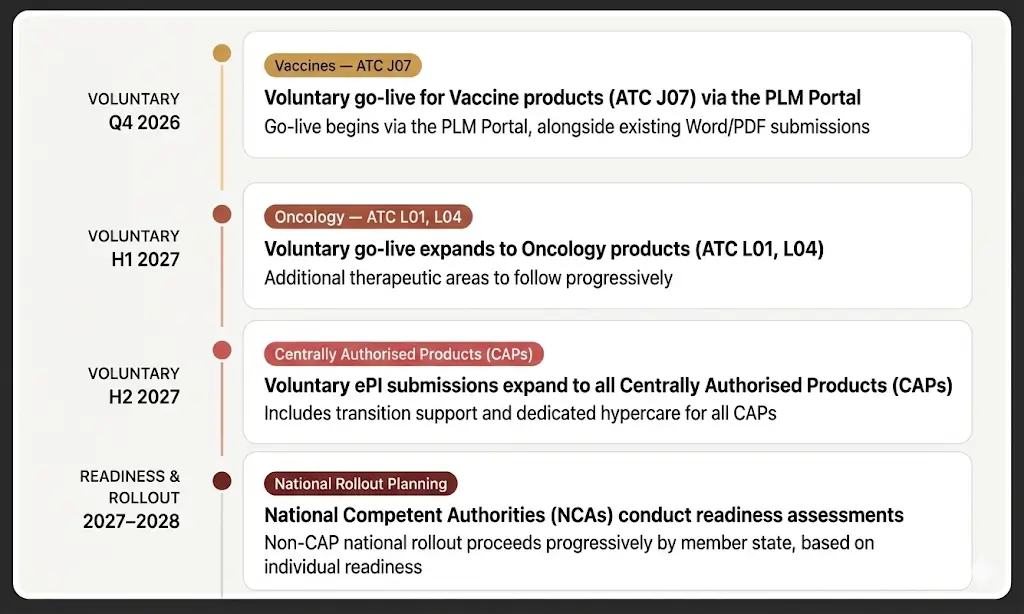
Figure 1: EMA ePI implementation sequence – voluntary phase transitioning to mandatory requirement post-legislation.
The question is not whether your organization will need to implement ePI. The question is whether you are building the capability now, while you have time to do it properly – or whether you will be forced into it under deadline pressure.
What EMA Requires Is Not a QR Code
A QR code linking to a PDF is not ePI compliance. EMA’s June 2025 reflection paper was explicit: the ePI initiative requires structured, FHIR-compliant product information – not a document link.
Real ePI compliance requires:
- SmPC, Package Leaflet, and labelling authored or converted as structured FHIR data
- Conformance to the EU FHIR EPI Implementation Guide
- A GxP-compliant audit trail on every conversion, authoring, and submission event
- Validated, submission-ready FHIR ePI resources that pass EU FHIR EPI IG validation before reaching the regulator.
The EMA Readiness Reality Check
Three questions. Answer them honestly — they determine whether your organization is genuinely on track for EMA compliance, or operating on assumptions that will not survive contact with your first deadline.
01. Do you know which products EMA’s timeline affects – and when?
EMA’s mandate moves by product category. If your team cannot map your portfolio against that sequence – by market, by format, by conversion complexity – you have an intention, not a programme.
02. Has your FHIR conversion been validated against the current EMA FHIR EPI IG?
The EMA FHIR EPI IG is an active document updated as the HL7 Vulcan EPI IG evolves. A conversion built against last quarter’s draft may fail against today’s specification – and rebuilds at the submission point are expensive.
03. Can you show leadership the compliance gap across your portfolio today?
Leadership approval requires data: how many labels, how many markets, what conversion complexity, against which deadlines. Portfolio-level visibility must exist before the programme is approved, not after
What a EMA – Ready Organisation Has Already Done
On track
- Completed a full label estate inventory mapped against EMA’s product category timeline
- Assessed cloud infrastructure against FHIR ePI requirements and GxP compliance standards
- Run a scoped Pathfinder conversion on one real label to validate the conversion path
- Built a conversion roadmap sequenced by EMA deadline – vaccines first, oncology next
At risk
- Treating a PDF export or QR code as an EMA ePI compliance answer
- Delegating FHIR architecture decisions to a generalist IT team without GxP experience
- Waiting for mandatory EMA deadlines before assessing conversion effort and complexity
- Building custom FHIR components without validating them against the current EMA FHIR EPI IG
Why Work With Deevita on Your EMA ePI Programme
Deevita’s team actively contributes to writing the HL7 Vulcan EPI Implementation Guide as Working Group members. We are inside the room where the standard is written – not reading it from the outside.
Deevita’s implementation architecture is built on Azure Health Data Services, giving your FHIR ePI infrastructure a validated, GxP-compatible cloud foundation that integrates with existing EU regulatory workflows – rather than a bespoke stack your team will need to maintain independently.
What that means for you: conformance requirements that change between working drafts do not surprise your programme. Your FHIR ePI resources are validated against the current specification – not last quarter’s. Your conversion investment is protected from the day it begins.
The Cost of Waiting Is Compounding
The earlier you begin, the more options you have – intelligent sequencing, piloting with one product, careful architecture decisions. The closer you get to mandatory deadlines without a programme in place, the fewer those options become and the more expensive every remaining one gets.
The Q3 2026 vaccine deadline is weeks away. The Q4 2026 oncology deadline follows immediately. The organisations that act in this window will have credible programmes and clear roadmaps. The ones that do not will be making decisions under exactly the kind of deadline pressure that drives costly mistakes.
Your Next Step Is One Conversation
Not sure where your organisation stands? A useful first move is to map your own exposure: how many of your products fall under vaccines (J07) or oncology (L01, L04), how many markets each label covers, and whether your current authoring environment produces FHIR output or documents.
Deevita’s ePI Readiness Assessment gives your regulatory team a complete, portfolio-level picture – products mapped against EMA’s timeline, conversion complexity scored, architecture gaps identified, and a business case structured for leadership approval. Most organisations complete the Assessment in two to three weeks.
